The 10 Meter Walk Test (10MWT) is one of the most widely used outcome measures in neurologic rehabilitation. It is quick to administer, requires little equipment, and provides a highly meaningful measure of walking speed, which has been described as the “sixth vital sign” because of its strong relationship with function, health status, and survival in adults (Middleton et al., 2015).
In this article we will discuss:
- Which patients should be assessed with the 10MWT
- How to administer the test in a standardized way
- Age-matched norms, minimal detectable change (MDC), and minimally clinically important difference (MCID), and how these values can predict functional status and guide goal writing
Part I: Which Patient Populations Are Appropriate to Assess With the 10MWT?
Within neurologic physical therapy practice, the 10MWT can be used with nearly any ambulatory patient who has goals related to improving walking ability. It has been validated across many neurological populations, including:
- Stroke
- Spinal cord injury
- Multiple sclerosis
- Traumatic brain injury
- Parkinson’s disease
The test measures walking speed in meters per second (m/s), which is strongly associated with functional mobility, community participation, and quality of life (Schmid et al., 2007).
Assistive devices and orthotics
Patients may use any assistive device or bracing required for safe ambulation, including walkers, canes, ankle–foot orthoses, or other orthotic supports. However, consistency is essential.
For example:
- If a patient uses a rolling walker at evaluation, they should use the same device during reassessment.
- If the patient progresses to a cane, it is best practice to first reassess using the walker for comparison with the initial test.
- Afterward, you may establish a new baseline 10MWT with the cane and write a new goal accordingly.
Always document the assistive device and bracing used during the test.
Providing assistance during the test
If the patient requires assistance for balance or safety, provide the minimum assistance necessary but document the highest level of assistance required during the trial.
Example:
If the patient was primarily standby assist but required minimal assist once to prevent loss of balance, the test should be documented as minimal assist.
When the 10MWT should not be used
The 10MWT is not recommended when the therapist must assist with forward propulsion, such as helping advance a hemiparetic limb.In these cases, walking speed becomes heavily influenced by the therapist’s timing and assistance, which reduces the reliability of the measure.
Part II: How to Correctly Administer the 10MWT
Standardized administration is important to ensure reliable and comparable results over time.
Establish the testing environment
Create a 10-meter walkway (32.8 ft) and mark the following points:
- Start
- 2 meters
- 8 meters
- 10 meters (finish)
The middle 6 meters are timed to eliminate the effects of acceleration and deceleration.
Test administration
It is recommended to perform:
- Two trials at comfortable walking speed (commonly referred to as self-selected velocity/SSV or comfortable gait speed/CGS)
- Two trials at fastest safe walking speed (fast velocity, FV)
For some patients early in rehabilitation or with medical limitations, it may be appropriate to perform only the self-selected velocity trials. Record the average of the two trials and report the final value in meters per second (m/s), by dividing 6 by the time in seconds.
Timing
Start the timer when any part of the leading foot crosses the 2-meter mark and stop the timer when the leading foot crosses the 8-meter mark.
Therapist positioning
To avoid unintentionally pacing the patient:
- Walk slightly behind the patient if possible
- Avoid walking beside or ahead of the patient
- Limit conversation during the test
For safety reasons, these recommendations may need modification.
If the patient is not yet ambulatory
If the patient cannot walk at evaluation but is expected to regain walking ability, it is acceptable to document a baseline gait speed of 0.0 m/s.
Patient Instructions
Self-selected velocity (SSV):
“When I say go, walk at your comfortable walking pace until I say stop.”
Fast velocity (FV):
“When I say go, walk at your fastest safe walking speed until I say stop.”
Part III: Normative Values, MDC, and MCID
Understanding normative values and meaningful change thresholds helps clinicians interpret results and write realistic goals.
Age-Matched Normative Walking Speeds
Average self-selected walking speeds for healthy adults are shown below (Bohannon & Williams Andrews, 2011).
|
Age
|
Men (speed in meters/sec)
|
Women (speed in meters/sec)
|
|
20s
|
1.358
|
1.341
|
|
30s
|
1.433
|
1.337
|
|
40s
|
1.434
|
1.390
|
|
50s
|
1.433
|
1.313
|
|
60s
|
1.339
|
1.241
|
|
70s
|
1.262
|
1.132
|
|
80s/90s
|
0.968
|
0.943
|
Interpreting Gait Speeds
Walking speed provides meaningful insight into a patient’s functional mobility.
For individuals after stroke, the following thresholds are commonly used (Perry et al., 1995):
|
Gait Speed
|
Functional Classification
|
|
<0.4m/s
|
Household ambulator
|
|
0.4-0.8m/s
|
Limited community ambulator
|
|
>0.8m/s
|
Community ambulator
|
Although developed in stroke populations, these thresholds are often applied broadly across neurological diagnoses.
Faster walking speeds have been associated with greater independence, higher community participation, and improved quality of life (Schmid et al., 2007).
Predicting Functional Outcomes Based on Walking Speed
Walking speed is more than just a measure of mobility. Research has shown that gait speed is strongly associated with important health and functional outcomes, including independence, fall risk, hospitalization, and mortality.
Because of these strong relationships, gait speed has been described as the “sixth vital sign” in adults. In a widely cited paper, Andrew Middleton, Stacey Fritz, and Mary Lusardi summarized evidence linking specific walking speed ranges with predicted functional outcomes.
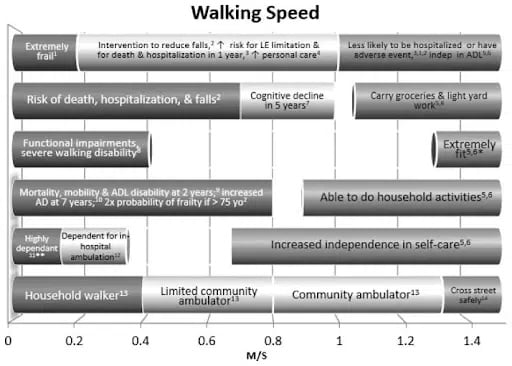
Table from Middleton, Fritz, & Lusardi (2015) summarizing the relationship between gait speed and functional outcomes.
Minimal Detectable Change (MDC) and Minimally Clinically Important Difference (MCID)
- Minimal Detectable Change (MDC): The smallest measurable change beyond measurement error.
- Minimally Clinically Important Difference (MCID): The smallest change perceived as meaningful by the patient.
Both values help clinicians determine whether an intervention is producing true improvement.
Stroke
Traditional values used in clinical practice:
MDC
- Acute: 0.11 m/s
- Chronic (>6 months), SSV: 0.18 m/s
- Chronic (>6 months), FV: 0.13 m/s
MCID
- Acute/subacute: 0.16 m/s
More recent research suggests MDC values may vary depending on baseline walking speed and provided the following MDCs based on a patient’s gait speed classification as low, moderate, or higher speed. (Hosoi et al., 2023):
| Gait Speed | SSV MDC | FV MDC |
| Low (<0.4m/s) | 0.05m/s | 0.04m/s |
| Moderate (0.4-0.8m/s) | 0.11m/s | 0.12m/s |
| High (>0.8m/s) | 0.21m/s | 0.19m/s |
This classification is helpful because individuals with very low baseline walking speeds may show meaningful progress with smaller improvements in gait speed.
Spinal Cord Injury
For individuals with spinal cord injury:
MDC (SSV)
≈ 0.06–0.105 m/s
MCID (SSV)
≈ 0.06–0.15 m/s
In individuals within the first year after injury, MDC values closer to 0.13 m/s have been reported.
There is currently limited research on fast walking speed (FV) changes in SCI.
Multiple Sclerosis
For individuals with EDSS scores 0–6.5:
MDC (SSV and FV)
≈ 0.26 m/s
Other outcome measures commonly used to assess walking in MS include:
- Timed 25-Foot Walk
- 6-Minute Walk Test
- Multiple Sclerosis Walking Scale–12
These tools may provide additional insight into mobility limitations.
Brain Injury
MDC:
≈ 0.05 m/s
MCID:
- SSV: 0.15 m/s
- FV: 0.25 m/s
Parkinson’s Disease
MDC
- SSV: 0.18 m/s
- FV: 0.25 m/s
Sample 10MWT Goals in Neurologic Rehabilitation
When writing goals based on the 10MWT, it is helpful to include:
- The baseline gait speed
- The target gait speed
- The assistive device or level of assistance
- A functional implication when possible
When writing goals, consider the available MDC and MCID values. MDC can help guide shorter-term goals that reflect measurable change, while MCID may be better suited for longer-term goals focused on meaningful functional improvement.
Below are several examples across different clinical scenarios.
Example 1: Improving Household Mobility
Goal: Patient will increase 10MWT Self Selected Velocity from 0.28 m/s to 0.40 m/s using a bilateral platform rolling walker with up to minimal assistance in order to improve household mobility and functional independence within 4 weeks.
Example 2: Transitioning to Community Ambulation
Goal: Patient will increase 10MWT Self Selected Velocity from 0.55 m/s to 0.75 m/s using a single-point cane and R AFO with no more than standby assist to increase safety and access when ambulating in less-crowded community environments within 6 weeks.
Example 3: Advancing Community Ambulation
Goal: Patient will increase10MWT Fast Velocity from 0.72 m/s to ≥0.90 m/s without an assistive device independently in order to progress toward safely crossing streets for community mobility and return to work activities within 6 weeks.
Key Takeaways
The 10MWT is a valuable tool because it is:
- Quick and easy to administer
- Highly reliable
- Clinically meaningful across neurologic diagnoses
When used consistently and interpreted with appropriate MDC and MCID values, it can help clinicians:
- Track recovery over time
- Determine treatment effectiveness
- Write measurable, patient-centered goals
References
Bohannon, R. W., & Williams Andrews, A. (2011). Normal walking speed: A descriptive meta-analysis. Physiotherapy, 97(3), 182–189. https://doi.org/10.1016/j.physio.2010.12.004
Hosoi, Y., Yoshida, T., Yamamoto, S., et al. (2023). Minimal detectable change for the 10-meter walk test based on gait speed classification in individuals with stroke. Journal of Clinical Medicine, 12(14), 4687. https://doi.org/10.3390/jcm12144687
Middleton, A., Fritz, S. L., & Lusardi, M. (2015). Walking speed: The functional vital sign. Journal of Aging and Physical Activity, 23(2), 314–322. https://doi.org/10.1123/japa.2013-0236
Perry, J., Garrett, M., Gronley, J., & Mulroy, S. (1995). Classification of walking handicap in the stroke population. Stroke, 26(6), 982–989. https://doi.org/10.1161/01.STR.26.6.982
Schmid, A., Duncan, P. W., Studenski, S., et al. (2007). Improvements in speed-based gait classifications are meaningful. Stroke, 38(7), 2096–2100. https://doi.org/10.1161/STROKEAHA.106.475921
Academy of Neurologic Physical Therapy. (2026). 10 Meter Walk Test: Core outcome measure pocket guide. https://neuropt.org
Shirley Ryan AbilityLab. (n.d.). 10 Meter Walk Test.https://www.sralab.org/rehabilitation-measures/10-meter-walk-testSCIRE Project. (n.d.). 10 Meter Walk Test.https://scireproject.com/outcome/10-meter-walk-test/


